
Muslim communities in Southeast Michigan and other parts of the United States experience discrimination and unequal access to health care (1–4). A 2022 survey by the Institute for Social Policy and Understanding (ISPU) showed that a majority (62%) of Muslims in America have experienced religious-based discrimination in the past year. Related to health care services and the healthcare system, American Muslims experience many challenges when seeking, accessing, and receiving health care services. Some of these challenges are due to sociopolitical context (i.e., the social, economic, and political conditions in their community), Islamophobia, and the lack of cultural competence of some healthcare professionals. The number and quality of studies to understand health disparities specifically among American Muslims is limited (4,6) yet growing. Despite this, Padela and Heisler (3) reported that perceived post-9/11 abuse and discrimination was associated with worse health statuses among Arab Americans living in the greater Detroit area. A systematic review by Samari, Alcalá, and Sharif (4) identified studies showing Islamophobia is associated with poor mental health, suboptimal health behaviors, and unfavorable health care-seeking behaviors. Interviews with community members, faith leaders, and mental health professionals in Southeast Michigan point to an increasing demand for mental health services partly due to Islamophobia (7).
Given this background, the purpose of this study was to empower Muslims in Southeast Michigan with the knowledge and tools to advocate for accessible, equitable, unbiased, and quality health care in their communities. Research-informed insights and accessible communication materials are the types of knowledge and tools that can be used by individuals, organizations, and others to advocate for equitable access to health care. The study focused on the following objectives:
Specifically, the systems approach helps communities identify which factors to address for closing gaps in outcomes (e.g., disparities in emergency department utilization between foreign-born Arab Americans and U.S.-born white Americans) or shifting outcomes in a positive direction (e.g., increasing the number of American Muslims who require mental health and addiction treatment who actually get into and complete treatment). The systems approach lends itself to addressing these complex challenges because multiple parts of the system must work together in a certain way to bring about the desired change in the system (e.g., closing gaps or shifting outcomes positively), which requires considering and implementing multiple policies rather than one single policy at multiple levels of organization (e.g., individual, interpersonal, family, neighborhood, community, county, state, and federal).
This study involved holding a series of workshops with community members, analyzing and summarizing the information shared by workshop participants, and communicating the main research findings back to community members and key stakeholders. The study setting was the following counties in the U.S. state of Michigan: Oakland, Wayne, Washtenaw, and Macomb. We recruited two types of participants: core modeling team members and workshop participants. Core modeling team members acted as a steering committee and helped guide the research team on the design of the workshops, identified and helped to recruit workshop participants, and reviewed study findings. Workshop participants shared with the research team their local knowledge and experience over the course of five workshops held from December 2023 to March 2024. We also interviewed community leaders to make sure that the study findings were relevant to ongoing community issues. The goal of the workshops was to address a problem statement developed by the workshop participants: “Which factors affect access to healthcare experienced by Muslim communities in Southeast Michigan?”
The recruitment process for the workshops was carried out in partnership with members of the steering committee and through individuals and organizations we identified after conducting a landscape analysis of public health and healthcare programs in the study setting. Seven individuals from diverse backgrounds participated in the workshops and 6 individuals participated in the one-on-one interviews. The workshop activities led to the development of several visualizations (e.g., key stakeholder graph), tables (e.g., policy options), and feedback loops (e.g., a visual representation of how two or more factors affect each other) that may be helpful for future advocacy efforts focused on equitable access to healthcare. These materials are available in the full report.
The study protocol received approval from the WCG Institutional Review Board (IRB) and was conducted in accordance with ethical guidelines for human subjects research.
The following recommendations are based on the information obtained and analyzed from the workshop activities and community interviews. These recommendations are intended for those who seek to advocate for accessible, equitable, unbiased, and quality health care in their communities in Southeast Michigan. The full version of these recommendations with supporting materials are available in the full report.
Recommendation #1: Design and implement new ways to increase the ability of American Muslims to access, afford, and trust the healthcare system. Stakeholders should pursue this goal while supporting ongoing efforts that address approachability (e.g., translation services), accommodation (e.g., halal status of food and medication), and appropriateness (e.g., care provided by a provider who is the same gender as the patient) of health care services.
Recommendation #2: Design and implement prevention strategies that prioritize the demographics, immigration experience, and socioeconomic makeup of neighborhoods. Neighborhoods are geographic areas perceived by residents who have a shared identity rather than arbitrary administrative boundaries (e.g., census tracts).
Recommendation #3: Address hard-to-reach and minoritized populations. State and city health and human service organizations (e.g., health departments, community action agencies), community health centers (e.g., federally qualified health centers, free clinics serving Muslims and other community groups), and community mental health agencies and treatment providers should build on existing partnerships and explore new opportunities that focus on innovative, diplomatic approaches to addressing health literacy, health misinformation, and health communication among hard-to-reach and minoritized populations.
Recommendation #4: Increase the number of Muslim community health workers (CHWs). Stakeholders can raise awareness of educational pathways to public health and healthcare professions and build sustainable collaborations with agencies who employ Muslim CHWs who are already serving American Muslim communities in Southeast Michigan.
Recommendation #5: Holistically address social determinants of health. Community-based organizations that assist Muslim patients and clients with health-related social needs, such as food insecurity, transportation, and rent assistance, should partner with the regional initiatives (e.g., Community Information Exchange, Wayne County Community Action Agency) to holistically address social determinants of health.
Recommendation #6: Build bridges with community organizations, healthcare systems, and local governments. Local Muslim religious centers and community-based organizations should continue to build intentional bridges with public and community health organizations, hospitals, community-based organizations, and city/county governments that focus on social determinants of health, access to care, and specific health outcomes, such as mental health, maternal and child health, chronic diseases, and elderly care.
The social determinants of health are defined by the Centers for Disease Control and Prevention and the World Health Organization as follows:
“Social determinants of health (SDOH) are the nonmedical factors that influence health outcomes. They are the conditions in which people are born, grow, work, live, and age. These forces and systems include a wide set of forces and systems that shape daily life such as economic policies and systems, development agendas, social norms, social policies, and political systems.” (8)
ACCESS: Arab Community Center for Economic and Social Services
CBO: Community-Based Organizations
CBSD: Community-Based System Dynamics
CHW: Community Health Worker
CIE: Community Information Exchange
CMT: Core Modeling Team
GMB: Group Model Building

This research was led by ISPU, in partnership with Huda Clinic.
Support for this research (grant #79552) was provided by the Robert Wood Johnson Foundation’s Community Research for Health Equity program, managed by AcademyHealth. The views expressed here do not necessarily reflect the views of the Foundation or AcademyHealth.
In addition to the support of our foundation partners, ISPU’s work is powered by individual donors. If work like this matters to you, consider a donation to ISPU today.
We conducted an exploratory mixed methods study using a combination of qualitative and quantitative methods through the lens of community-engaged research. For Objectives 1 and 2, we used a community-based system dynamics (CBSD) approach. CBSD is a set of methods including facilitated group discussions in a workshop format, a qualitative analysis of the diagrams and written content generated from the workshops, and a quantitative model of the relationship between factors related to the problem statement and based on the qualitative analysis. The problem statement was developed by the workshop participants. For Objective 3, we extended a civic empowerment model to disseminate research findings among different stakeholder types. The timeframe for completing the study was three years, starting in May of 2022.
The study setting was Oakland, Wayne, Washtenaw, and Macomb Counties in Michigan. These counties were selected based on data from the U.S. Census on Religion 2020 that showed a high concentration of American Muslims living in these counties. In Wayne County, Islam is the largest non-Christian religion with about 79,266 adherents. In Oakland County, Islam has around 33,125 adherents. In Macomb County, there are an estimated 24,850 Muslims. In Washtenaw County, the Muslim population is approximately 9,445 (21). Furthermore, members of our project team have previously collaborated on ISPU initiatives with the American Muslim community in Michigan, such as the report on Muslim contributions to Michigan (22). For these two reasons, the study team decided to explore the application of a systems approach to community empowerment in Southeast Michigan.
We recruited two types of participants using the following recruitment strategy. The first type of participants were members of the Core Modeling Team (CMT); the second type were those who attended the Group Model Building (GMB) workshops. A CMT is a local steering committee that guides the design of the research, champions the research with the local community, and provides local context for the appropriate interpretation of research findings. During the GMB workshops, we engaged community participants in a series of facilitated group activities. We used a purposeful sampling approach to recruit both types of participants with an expectation of recruiting up to 5 participants to be members of the local steering committee and up to 15 individuals to participate in the workshops. These sample sizes are the norm when implementing the CBSD approach (18, 23). In addition, the inclusion criteria for both activities were as follows: residing in at least one of the four counties in the study area or serving the American Muslim communities in the study area, being 18 years of age or older, and having the ability to speak English. Additional criteria were used to identify potential workshop participants (see Supplementary Materials).
Based on these criteria, we first assembled the local steering committee by using a recruitment script sent by email (see Supplementary Materials). We sent this email to our two study partners, the HUDA Clinic and ACCESS (Arab Community Center for Economic and Social Services), and asked them to identify additional names of people who might be suitable for the steering committee. Based on the list of names we received from the study partners, we recruited one additional committee member. All local steering committee members were required to sign an informed consent form.
HUDA Clinic (Health Unit on Davison Avenue)
A free community health clinic located in Detroit, MI, that serves mainly uninsured, underinsured, and publicly insured patients and provides primary care, dental, vision care, podiatry, and mental health services
ACCESS (Arab Community Center for Economic and Social Services)
A community-based organization with locations concentrated in Dearborn, MI, that provides community-based health care services, integrated behavioral health, and a range of educational programs that focus on disease prevention and health promotion
Some of the eligible workshop participants were leaders in government or community health. These individuals did not have the capacity to participate in the four workshops due to other commitments. Therefore, we engaged these individuals using a semi-structured interview format. The analysis and insights in this report are provided separately for the workshops and the interviews.
It is important to note that due to a variety of reasons, which we elaborate on in the insights section below, we undertook a targeted recruitment approach to engage Black Muslims using the same inclusion criteria above with the additional criteria of being racialized as Black. Our recruitment efforts involved reaching out to key influential leaders and community members in the local African American community, setting up a separate set of workshops that would be facilitated by an African American leader, and extending the recruitment period. It was important to make this effort because the lived experience of racialized individuals, whether Black, South Asian, or Arab American, are not the same, regardless of whether they share the same religious identity. Despite these efforts, we were only able to recruit two African American Muslim leaders for this study. One individual participated in the workshops, and another individual participated in an interview.
The study protocol received approval from the WCG Institutional Review Board (IRB) and was conducted in accordance with ethical guidelines for human subjects research.
The local steering committee had four members: three committee members were administrators from the HUDA Clinic (n=2) and ACCESS (n=1) and one was a local community leader with a health research background. The committee met four times over the course of the study. A charter and a communication plan was developed to take into account the capacity and interests of the steering committee members. The meetings focused on gathering feedback on the format and timeline of the workshops, identifying potential workshop participants, reviewing the initial findings of the workshops, and gathering insights on dissemination strategies. Local steering committee members were compensated at a rate of $50/meeting.
Potential participants (n=28) were invited to attend the workshops based on the participant recruitment strategy. Initially, 10 individuals agreed to attend but, ultimately, 7 individuals attended the four workshops, which were held in-person (workshop #1, #3, and #4) and online (workshop #2). Some of the reasons given by those who initially agreed to participate but then backed out were misunderstanding the time commitment, lack of childcare, change in job status, and limited availability on weekends.
The workshops consisted of individuals from diverse backgrounds based on ethnicity, race, and professional experience. Out of the seven participants, three were women and four were men, four were South Asian, two were Arab, and one was African American. One participant was from the education sector, three participants were from the healthcare sector, two participants were medical students, and one participant was in public health administration. Three of the participants held senior or executive-level positions within their place of work.
We organized four half-day long workshops from December 2023 to March 2024 (i.e., every second Saturday of the month) and participants were compensated $100 for each workshop.The purpose of these workshops was to generate new insights using systems thinking and system dynamics. Systems thinking is a way of thinking about the parts of a system and how they interact with each other to change the larger system. In the context of access to health care, the parts of the system are the factors associated with access to health care, and the larger system consists of access to health care services and the healthcare system. Based on this example, system dynamics is the way in which the system shifts in response to changes in some or all parts of the system (e.g., lower trust in a health care provider results in less chances of a patient coming back to that provider, higher levels of racial discrimination by a public health system leads to a decrease in the level of trust placed in the public health system by individuals or whole communities). The workshop activities and outputs (digital versions) are available in the Supplementary Materials. Workshop outputs in the main text of the report are intended to be examples and readers who want to view the diversity of workshop outputs should review the entire Supplementary Materials document. The facilitation guide for the first workshop (see Supplementary Materials) might be helpful for others interested in applying our approach to a complex and challenging topic facing their community.
In addition to the workshops, we conducted semi-structured interviews online with leaders in government and community health. The purpose of these interviews was two-fold. First, we validated some of the findings from workshop #1 regarding the problem statement, initial policy options, and key stakeholders. Validating these workshop outputs with the interviewees was important because the sectors they represented were not included in the workshops. For example, although we had a workshop participant who was a public health leader at a county health department, the perspective of a local health department leader was missing from the workshop. Similarly, we did not have anyone who represented the perspective of the City of Detroit and, therefore, interviewing an individual who worked in a public health-adjacent role within the City of Detroit was important to include in the study. The format of the interview was as follows. We presented to interviewees an overview of the project and digital versions of the outputs from workshop #1. We asked interviewees to review the materials presented for anything that was missing, should be added, or needed clarification based on the problem statement finalized by the workshop participants.

We created a digital version of outputs from each workshop activity and added relevant information, such as the number of votes, as applicable. For some activities, such as reviewing the feedback loops, we supplemented the digital version of each loop with relevant programs and initiatives based on the landscape analysis and participant input. Additionally, we derived insights from each of the workshop outputs and gathered data from multiple sources to corroborate the insights. The data sources we reviewed included the 2020 Decennial Census and American Community Survey from the U.S. Census Bureau, the PLACES data from the Centers for Disease Control, Area Health Resource File from the Health Resources and Services Administration, and the Environmental Justice Index from the Environmental Protection Agency. Using these sources, we developed a map highlighting multiple layers of information, including the locations of mosques in Southeast Michigan (a proxy measure for the residence of Muslim populations), areas of high social vulnerability, and limited access to healthcare services.
We recorded each online interview, and study team members summarized the responses of interviewees in a written document. In workshop #3, we presented these summary responses to the workshop participants along with information on the names, titles, and organizational affiliations of the interviewees. The workshop participants had the final say in what pieces of information and suggestions from the interviewees should be used to revise workshop outputs. This approach for integrating perspective between workshop participants and interviewees who did not attend the four workshops honored and prioritized the perspectives of workshop participants.
Tables S2 and S3 in the Supplementary Materials provide an overview of the activities conducted within each workshop including the purpose and output(s) of each activity. The following narrative summary identifies the main insights from workshop activities. We first identified the hopes and fears of workshop participants regarding this study. While the participants were hopeful that the overall study would have a practical and positive impact, they also feared that it lacked relevance to the broader community and that its scope and impact would be limited. In particular, participants raised concerns that an insufficient number of sectors were being represented among the workshop participants. For example, leaders or representatives from nonprofit organizations, patients and family advocates, immigrant and refugee communities, and policymakers were not represented in the workshops.
The problem statement for the workshops was “Which factors affect access to healthcare experienced by Muslim communities in Southeast Michigan?.” This statement was broad in scope and developed by workshop participants (Table S1 in Supplementary Materials), which might reflect the additional space participants wanted to give themselves since they feared that an insufficient number of sectors were represented at the workshop.
The problem statement developed by workshop participants: “Which factors affect access to healthcare experienced by Muslim communities in Southeast Michigan?”
As a result of the broad scope of the problem statement, it was not surprising that the participants came up with 36 key stakeholders with varying levels of power and interest to address their problem statement (Fig. 1). Prominent categories of key stakeholders included elected officials (e.g., City of Detroit Mayor Mike Duggan), healthcare systems and community health centers (e.g., Detroit Wayne Integrated Health System, Henry Ford Health), social and human service providers (e.g., Zaman International, Gleaners Food Bank), advocacy groups and community-based organizations (e.g., CAIR Michigan, Muhsen), and educational institutions (e.g., Miftaah Institute, local Muslim Students Association chapters). The interpretation of key stakeholders with low interest and high power (e.g., local media) is that these stakeholders have little interest or concern for the problem statement (i.e., factors associated with access to healthcare experienced by Muslim communities in Southeast Michigan). On the other hand, these stakeholders have high levels of power and influence over the factors associated with access to healthcare and could effectively and quickly address those factors.
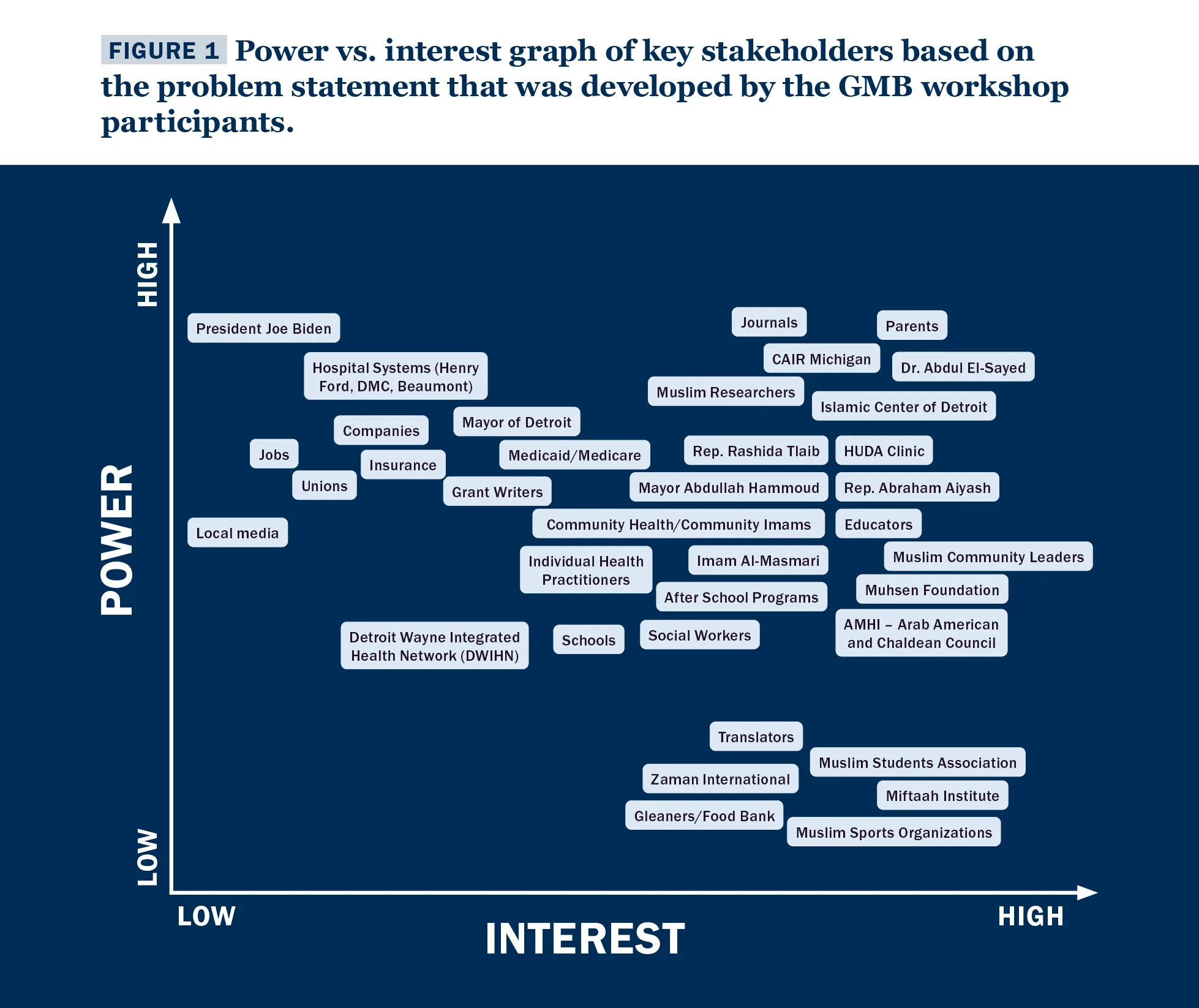 Figure 1. Power vs. interest graph of key stakeholders based on the problem statement that was developed by the GMB workshop participants. Power in this context refers to the level of agency and influence, and interest refers to the level of interest of the key stakeholder to directly or indirectly address the problem.
Figure 1. Power vs. interest graph of key stakeholders based on the problem statement that was developed by the GMB workshop participants. Power in this context refers to the level of agency and influence, and interest refers to the level of interest of the key stakeholder to directly or indirectly address the problem.
This graph provided three key insights:
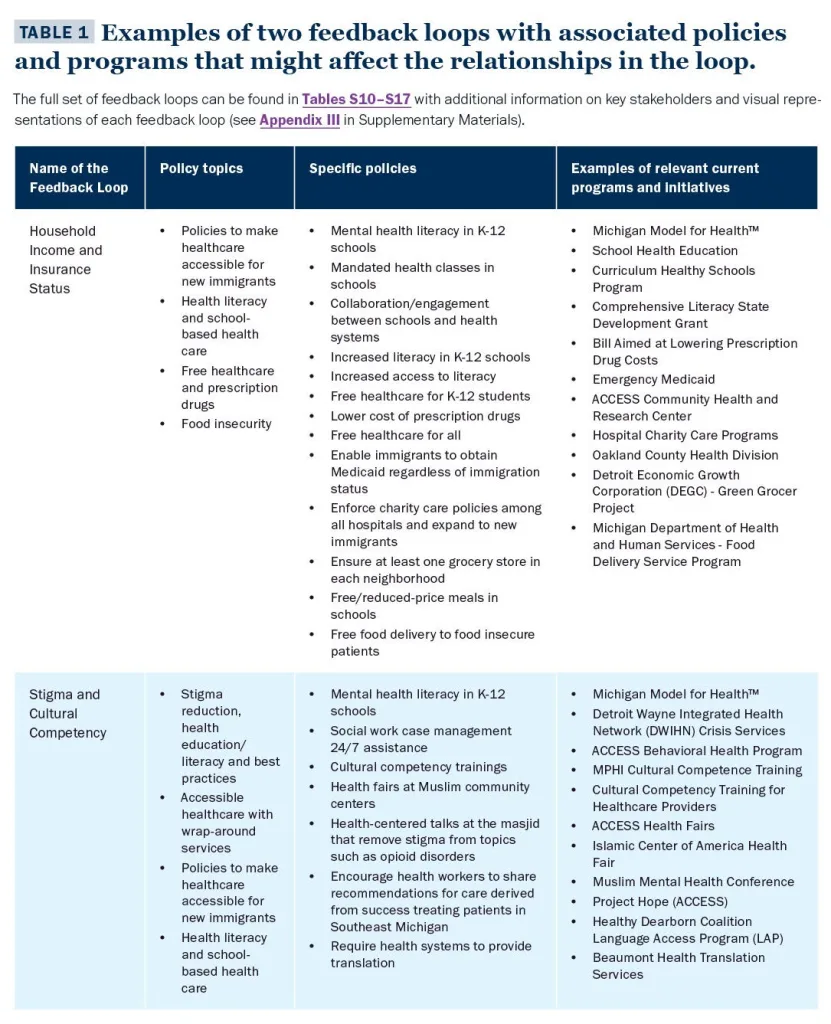
Based on the problem statement and key stakeholders, the workshop participants came up with 26 initial policy options that key stakeholders might consider to address the problem statement, including promoting mental health literacy in K-12 schools, enabling immigrants to obtain Medicaid regardless of their immigration status, enforcing charity care policies among all hospitals and expanding to new immigrants, offering free/reduced-price meals in schools, and free food delivery to food insecure patients. These policies were grouped into eight broader policy topics. For examples of policy topics, see Table 3; for a full list of policy topics and specific policies, see Tables S10 – S17 in Appendix III. After reviewing these broader policy topics, it became clear that the participants had identified policies that fit into either the social determinants of health or the public health/healthcare system. The public health system includes local and state health departments that strive to promote and protect the health of individuals and communities to give them a safe place to live, learn, work, play, and pray. The healthcare system includes hospitals, free clinics, and community health centers that serve the medical needs of patients in emergency, outpatient, and inpatient settings.
While some of the policies (see see Tables S10 – S17 in Appendix III) might seem unlikely or unrealistic, they served to highlight how we might address the problem rather than how we are currently addressing the problem of access to health care. This distinction is important because closing gaps in outcomes (e.g., disparities in emergency department utilization between foreign-born Arab Americans and U.S.-born white Americans) or shifting outcomes in a positive direction (e.g., increasing the number of American Muslims receiving mental health treatment) requires multiple parts of the larger system to work together by considering and implementing a range of policies rather than one single policy.
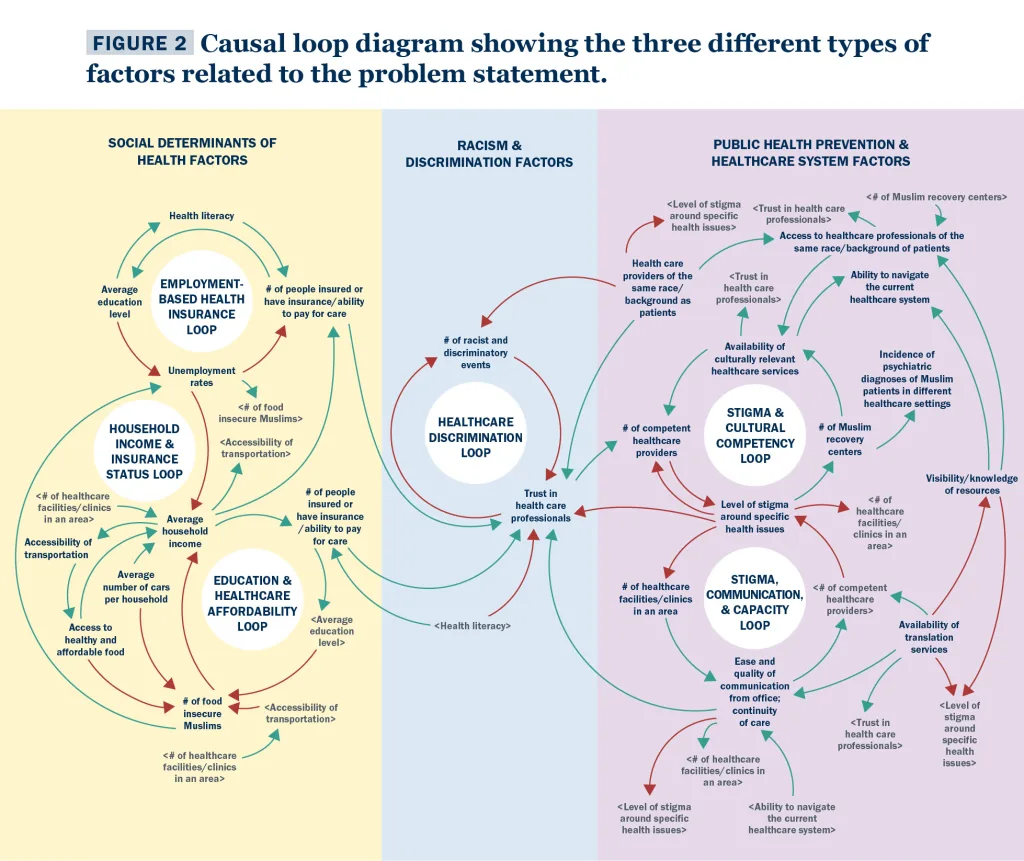
Participants identified variables of interest (see Table S7 and Fig. 2) that might be relevant to the key stakeholders and could be measured to see the impact of specific policies. Variables were identified through a series of workshop activities, such as the connection circle exercise. The relationships between these variables were organized visually in a causal loop diagram (Fig. 2). To better understand how to read this diagram, consider the example of the employment-based health insurance loop (top left in Fig. 2). This loop essentially suggests the following set of the statements:
The causal loop diagram was used to identify multiple feedback loops, and each feedback loop was named by workshop participants. Workshop participants also linked policies to feedback loops. This was an important linkage because it helps key stakeholders identify how they might slow or break down a feedback loop that leads to negative outcomes (e.g., in the employment-based health insurance loop example, rising unemployment rates would negatively affect the number of people insured through an employer). Table 3 provides examples of two feedback loops and related policies, key stakeholders, and existing programs/initiatives. Tables S10 – S17 in Appendix III provide similar information for all the feedback loops identified in the workshops.
The information in Tables S10 – S17 in Appendix III simplifies the complexity of the causal loop diagram (Fig. 2) into meaningful and easy-to-understand language for key stakeholders. One way to understand the information in Table 3, and similarly the more complete version in Tables S10 – S17 in Appendix III, is as follows.
Several insights emerged from reviewing the feedback loops and associated policies in Tables S10 – S17 in Appendix III and Figure 2.
First, there were three main categories of feedback loops: social determinants of health, racism and discrimination, and public health prevention and healthcare systems factors. These three types of feedback loops were different yet similar. They were distinct in the sense that different sets of key stakeholders might be interested in addressing them. For example, food banks, community-based organizations, and social service agencies would be more likely to address the social determinants of health and work with local mosques and Islamic centers than healthcare systems that lack the resources to address social determinants of health. The types of feedback loops were similar in the sense that there was overlap in policies (e.g., access to healthcare and health literacy) and relevant current programs and initiatives (e.g., Michigan Model for Health and ACCESS) needed to break the cycle of negative outcomes due to feedback loops. The key takeaway from this insight is that there are multiple pathways to address an outcome or variable of interest to American Muslim communities and key stakeholders in the health and healthcare system. The challenge is to identify those outcomes or variables of mutual interest and use the information in Tables S10 – S17 in Appendix III and Figure 2 to develop a shared understanding of which pathway to follow (i.e., which feedback loop to focus on). Once this shared understanding exists by clearly identifying the feedback loop(s) of interest, then it might be possible to identify existing programs and initiatives or develop new ones to collaboratively address the outcomes of mutual interest. This is one example of how a system approach might help American Muslim communities address big, complex challenges.
Second, the variable “trust in health care professionals” was the only common variable across the three types of feedback loops. This is not surprising and has been found in several other studies focusing on American Muslims (15, 23–26), the general public (27), and minoritized populations (28,29). Among American Muslims, the diversity of their backgrounds and experiences with discrimination due to race, ethnicity, religious practice and clothing, gender, sex, legal status, and socioeconomic status also plays a role when it comes to trust in health care professionals.
The central importance of trust in health care professionals provides an important insight from a systems perspective—it is insufficient for key stakeholders to address only one type of feedback loop. Instead, all feedback loops should be addressed to the extent possible. This is best illustrated by imagining a tricycle. The tricycle only moves forward as fast as it can when all three wheels are rotating in the same direction and at the same time. If two wheels are moving forward and the third wheel is moving backward or not moving at all, then there might be some progress in the right direction, but it is not moving as quickly as it would if the third wheel was also moving in the forward direction.
Applying this analogy to the three feedback loops (i.e., the wheels), it is easier to see that key stakeholders must address all three types of feedback loops: social determinants of health AND racism and discrimination AND public health prevention and healthcare systems factors. Addressing only the social determinants of health, for example, will increase trust in health care professionals but not as much as when stakeholders also address the other two types of feedback loops. While this is the ideal scenario, the lived experience of communities is often not ideal. Therefore, it is best for a community to address the three types of feedback loops at the same time to whatever extent possible based on their level of resources and capacity instead of addressing only one type of feedback loop or addressing the feedback loops in a sequence (e.g., first addressing social determinants of health, second racism and discrimination, and last public health prevention and healthcare factors).
Lastly, we identified specific key stakeholders who might be able to address the feedback loops in this study through specific current policies or programs. Tables S10 – S17 in Appendix III provide a comprehensive list of such policies and key stakeholders for each of the six feedback loops that were identified by workshop participants. The format of this information provides a customized way to share research findings back with the community and makes it easy for them to access the research and advocate to key stakeholders in a sustainable and practical manner. There are several ways different key stakeholders may use the information in Tables S10 – S17 in Appendix III to be empowered as a Muslim community in Southeast Michigan with sustainable and practical tools to advocate for solutions to healthcare access.
In addition to the GMB workshops, the insights from interviews with leaders in government and community health added important nuance and additional insights apart from what was learned from the workshop participants. Furthermore, the interviewees validated the workshop outputs, which was reassuring given the smaller than intended sample size of the GMB workshops. The following quotes capture their excitement for the project.
“Wonderful—[a] generational loop that needs to be broken such as stigma, so excited for this effort. ” —Quote from an interviewee
“Impressed with the scope—detailed, broad range of policy outcomes, rooted in community, built on the experiences of people. Intrigued.” —Quote from an interviewee
Interviewees identified some important key stakeholders such as ACCESS, Dearborn Department of Public Health, foundations and funders (e.g., Kresge Foundation, Ford Foundation), American Moslem Society (in Dearborn, MI), and Wayne Regional Educational Service Agency. Interviewees also identified several additional policy categories and specific policies including the following:
These insights added nuance to the feedback from the workshop. The suggestion of health diplomacy as a policy option, while similar, was distinct from the suggestion by workshop participants for health literacy as a policy option. While health diplomacy and health literacy fall under health communication, who practices them and in what setting is nuanced and important to highlight for American Muslims. Health diplomacy has to do with how, who, when, and what health information, programs, and policies are communicated to the public; health literacy focuses more so on the comprehension of the audience receiving the health information. Based on the feedback from the interviewees, health diplomacy seems to be more important for leaders in public health and healthcare, whereas health literacy was important to care coordinators, community managers, and community health workers. In Southeast Michigan where American Muslims are in positions of public health and healthcare leadership, a greater emphasis on health diplomacy might be more important than in other parts of the U.S. where American Muslims are not in such leadership positions. In this latter setting, health literacy would be the policy option with the greatest impact compared to health diplomacy.
Another nuance, which was not surprising given that the interviewees were public health leaders, was the identification of public health and healthcare organizations. Casting a wider net on the experience and level of organization where interviewees were situated within an organization enabled the identification of additional key stakeholders. These key stakeholders—such as ACCESS, Dearborn Department of Public Health, and foundations and funders—likely have high power and high interest but are not necessarily connected to those with similar levels of power and interest that were identified by workshop participants. The nuance here is that sometimes even leaders in public health, healthcare, mental health, and other spaces might not be aware of connections to other organizations with shared values and populations of interest. Not knowing which programs and initiatives are available or being organized by other organizations working within the same geographic region is a common issue in multiple sectors. The workshop outputs from this study might urgently help to address this issue by linking programs and initiatives to specific policies, stakeholders and feedback loops (Tables S10 – S17 in Appendix III). This would raise greater awareness among more key stakeholders regarding how best to leverage existing resources and programs to address inequities in access to health care among American Muslims in Southeast Michigan.

Taking these insights together from workshop participants and community leaders, we have the following recommendations for American Muslim communities in Southeast Michigan, particularly Arab American and South Asian populations, as they advocate for and seek to access, use, and receive high-quality healthcare.
Recommendation #1: Design and implement new ways to increase the ability of American Muslims to access, afford, and trust the healthcare system. Stakeholders should pursue this goal while supporting ongoing efforts that address approachability (e.g., translation services), accommodation (e.g., halal status of food and medication), and appropriateness (e.g., care provided by a provider the same gender as the patient) of health care services. For example, it is not simply the availability of translation services but the ability of patients to engage with the healthcare system through translators that should be the priority of healthcare systems and translation service providers. Similarly, the ease and quality of communication between healthcare office staff and patients is just as important as the religious accommodations for Muslim patients (e.g., gender concordant care).
Recommendation #2: Design and implement prevention strategies that prioritize the demographics, immigration experience, and socioeconomic makeup of neighborhoods. Neighborhoods are geographic areas perceived by residents who have a shared identity, rather than arbitrary administrative boundaries (e.g., census tracts). We provide suggestions of existing strategies that may be implemented to address specific feedback loops (see Tables S10 – S17 in Appendix III).
Recommendation #3: Address hard-to-reach and minoritized populations. State and city health and human service organizations (e.g., health departments, community action agencies), community health centers (e.g., federally qualified health centers, free clinics serving Muslims and other community groups), and community mental health agencies and treatment providers should build on existing partnerships and explore new opportunities that focus on innovative, diplomatic approaches to addressing health literacy, health misinformation, and health communication among hard-to-reach and minoritized populations. This might be accomplished through strengthening capacity to support health fairs, webinars, and educational initiatives at mosques, cultural centers, and other centers of community.
Recommendation #4: Increase the number of Muslim community health workers (CHWs). Stakeholders can raise awareness of educational pathways to public health and healthcare professions and build sustainable collaborations with agencies who employ Muslim CHWs who are already serving Southeast Michigan American Muslim communities. CHWs are often trusted individuals within the communities they serve.
Recommendation #5: Holistically address social determinants of health. Community-based organizations that assist Muslim patients and clients with health-related social needs, such as food insecurity, transportation, and rent assistance, should partner with the regional initiatives (e.g., Community Information Exchange, Wayne County Community Action Agency) to holistically address social determinants of health.
Recommendation #6: Build bridges with community organizations, healthcare systems, and local governments. Local Muslim religious centers and community-based organizations should continue to build intentional bridges with public and community health organizations, hospitals, community-based organizations, and city/county governments that focus on social determinants of health, access to care, and specific health outcomes, such as mental health, maternal and child health, chronic diseases, and elderly care.

Muslim communities in Southeast Michigan and other parts of the United States experience discrimination and unequal access to health care (1–4). A 2022 survey by the Institute for Social Policy and Understanding (ISPU) showed that a majority (62%) of Muslims in America have experienced religious-based discrimination in the past year. Related to health care services and the healthcare system, American Muslims experience many challenges when seeking, accessing, and receiving health care services. Some of these challenges are due to sociopolitical context (i.e., the social, economic, and political conditions in their community), Islamophobia, and the lack of cultural competence of some healthcare professionals. The number and quality of studies to understand health disparities specifically among American Muslims is limited (4,6) yet growing. Despite this, Padela and Heisler (3) reported that perceived post-9/11 abuse and discrimination was associated with worse health statuses among Arab Americans living in the greater Detroit area. A systematic review by Samari, Alcalá, and Sharif (4) identified studies showing Islamophobia is associated with poor mental health, suboptimal health behaviors, and unfavorable health care-seeking behaviors. Interviews with community members, faith leaders, and mental health professionals in Southeast Michigan point to an increasing demand for mental health services partly due to Islamophobia (7).
Given this background, the purpose of this study was to empower Muslims in Southeast Michigan with the knowledge and tools to advocate for accessible, equitable, unbiased, and quality health care in their communities. Research-informed insights and accessible communication materials are the types of knowledge and tools that can be used by individuals, organizations, and others to advocate for equitable access to health care. The study focused on the following objectives:
Specifically, the systems approach helps communities identify which factors to address for closing gaps in outcomes (e.g., disparities in emergency department utilization between foreign-born Arab Americans and U.S.-born white Americans) or shifting outcomes in a positive direction (e.g., increasing the number of American Muslims who require mental health and addiction treatment who actually get into and complete treatment). The systems approach lends itself to addressing these complex challenges because multiple parts of the system must work together in a certain way to bring about the desired change in the system (e.g., closing gaps or shifting outcomes positively), which requires considering and implementing multiple policies rather than one single policy at multiple levels of organization (e.g., individual, interpersonal, family, neighborhood, community, county, state, and federal).
This study involved holding a series of workshops with community members, analyzing and summarizing the information shared by workshop participants, and communicating the main research findings back to community members and key stakeholders. The study setting was the following counties in the U.S. state of Michigan: Oakland, Wayne, Washtenaw, and Macomb. We recruited two types of participants: core modeling team members and workshop participants. Core modeling team members acted as a steering committee and helped guide the research team on the design of the workshops, identified and helped to recruit workshop participants, and reviewed study findings. Workshop participants shared with the research team their local knowledge and experience over the course of five workshops held from December 2023 to March 2024. We also interviewed community leaders to make sure that the study findings were relevant to ongoing community issues. The goal of the workshops was to address a problem statement developed by the workshop participants: “Which factors affect access to healthcare experienced by Muslim communities in Southeast Michigan?”
The recruitment process for the workshops was carried out in partnership with members of the steering committee and through individuals and organizations we identified after conducting a landscape analysis of public health and healthcare programs in the study setting. Seven individuals from diverse backgrounds participated in the workshops and 6 individuals participated in the one-on-one interviews. The workshop activities led to the development of several visualizations (e.g., key stakeholder graph), tables (e.g., policy options), and feedback loops (e.g., a visual representation of how two or more factors affect each other) that may be helpful for future advocacy efforts focused on equitable access to healthcare. These materials are available in the full report.
The study protocol received approval from the WCG Institutional Review Board (IRB) and was conducted in accordance with ethical guidelines for human subjects research.
The following recommendations are based on the information obtained and analyzed from the workshop activities and community interviews. These recommendations are intended for those who seek to advocate for accessible, equitable, unbiased, and quality health care in their communities in Southeast Michigan. The full version of these recommendations with supporting materials are available in the full report.
Recommendation #1: Design and implement new ways to increase the ability of American Muslims to access, afford, and trust the healthcare system. Stakeholders should pursue this goal while supporting ongoing efforts that address approachability (e.g., translation services), accommodation (e.g., halal status of food and medication), and appropriateness (e.g., care provided by a provider who is the same gender as the patient) of health care services.
Recommendation #2: Design and implement prevention strategies that prioritize the demographics, immigration experience, and socioeconomic makeup of neighborhoods. Neighborhoods are geographic areas perceived by residents who have a shared identity rather than arbitrary administrative boundaries (e.g., census tracts).
Recommendation #3: Address hard-to-reach and minoritized populations. State and city health and human service organizations (e.g., health departments, community action agencies), community health centers (e.g., federally qualified health centers, free clinics serving Muslims and other community groups), and community mental health agencies and treatment providers should build on existing partnerships and explore new opportunities that focus on innovative, diplomatic approaches to addressing health literacy, health misinformation, and health communication among hard-to-reach and minoritized populations.
Recommendation #4: Increase the number of Muslim community health workers (CHWs). Stakeholders can raise awareness of educational pathways to public health and healthcare professions and build sustainable collaborations with agencies who employ Muslim CHWs who are already serving American Muslim communities in Southeast Michigan.
Recommendation #5: Holistically address social determinants of health. Community-based organizations that assist Muslim patients and clients with health-related social needs, such as food insecurity, transportation, and rent assistance, should partner with the regional initiatives (e.g., Community Information Exchange, Wayne County Community Action Agency) to holistically address social determinants of health.
Recommendation #6: Build bridges with community organizations, healthcare systems, and local governments. Local Muslim religious centers and community-based organizations should continue to build intentional bridges with public and community health organizations, hospitals, community-based organizations, and city/county governments that focus on social determinants of health, access to care, and specific health outcomes, such as mental health, maternal and child health, chronic diseases, and elderly care.
The social determinants of health are defined by the Centers for Disease Control and Prevention and the World Health Organization as follows:
“Social determinants of health (SDOH) are the nonmedical factors that influence health outcomes. They are the conditions in which people are born, grow, work, live, and age. These forces and systems include a wide set of forces and systems that shape daily life such as economic policies and systems, development agendas, social norms, social policies, and political systems.” (8)
ACCESS: Arab Community Center for Economic and Social Services
CBO: Community-Based Organizations
CBSD: Community-Based System Dynamics
CHW: Community Health Worker
CIE: Community Information Exchange
CMT: Core Modeling Team
GMB: Group Model Building
This research was led by ISPU, in partnership with Huda Clinic.
Support for this research (grant #79552) was provided by the Robert Wood Johnson Foundation’s Community Research for Health Equity program, managed by AcademyHealth. The views expressed here do not necessarily reflect the views of the Foundation or AcademyHealth.
In addition to the support of our foundation partners, ISPU’s work is powered by individual donors. If work like this matters to you, consider a donation to ISPU today.
We conducted an exploratory mixed methods study using a combination of qualitative and quantitative methods through the lens of community-engaged research. For Objectives 1 and 2, we used a community-based system dynamics (CBSD) approach. CBSD is a set of methods including facilitated group discussions in a workshop format, a qualitative analysis of the diagrams and written content generated from the workshops, and a quantitative model of the relationship between factors related to the problem statement and based on the qualitative analysis. The problem statement was developed by the workshop participants. For Objective 3, we extended a civic empowerment model to disseminate research findings among different stakeholder types. The timeframe for completing the study was three years, starting in May of 2022.
The study setting was Oakland, Wayne, Washtenaw, and Macomb Counties in Michigan. These counties were selected based on data from the U.S. Census on Religion 2020 that showed a high concentration of American Muslims living in these counties. In Wayne County, Islam is the largest non-Christian religion with about 79,266 adherents. In Oakland County, Islam has around 33,125 adherents. In Macomb County, there are an estimated 24,850 Muslims. In Washtenaw County, the Muslim population is approximately 9,445 (21). Furthermore, members of our project team have previously collaborated on ISPU initiatives with the American Muslim community in Michigan, such as the report on Muslim contributions to Michigan (22). For these two reasons, the study team decided to explore the application of a systems approach to community empowerment in Southeast Michigan.
We recruited two types of participants using the following recruitment strategy. The first type of participants were members of the Core Modeling Team (CMT); the second type were those who attended the Group Model Building (GMB) workshops. A CMT is a local steering committee that guides the design of the research, champions the research with the local community, and provides local context for the appropriate interpretation of research findings. During the GMB workshops, we engaged community participants in a series of facilitated group activities. We used a purposeful sampling approach to recruit both types of participants with an expectation of recruiting up to 5 participants to be members of the local steering committee and up to 15 individuals to participate in the workshops. These sample sizes are the norm when implementing the CBSD approach (18, 23). In addition, the inclusion criteria for both activities were as follows: residing in at least one of the four counties in the study area or serving the American Muslim communities in the study area, being 18 years of age or older, and having the ability to speak English. Additional criteria were used to identify potential workshop participants (see Supplementary Materials).
Based on these criteria, we first assembled the local steering committee by using a recruitment script sent by email (see Supplementary Materials). We sent this email to our two study partners, the HUDA Clinic and ACCESS (Arab Community Center for Economic and Social Services), and asked them to identify additional names of people who might be suitable for the steering committee. Based on the list of names we received from the study partners, we recruited one additional committee member. All local steering committee members were required to sign an informed consent form.
HUDA Clinic (Health Unit on Davison Avenue)
A free community health clinic located in Detroit, MI, that serves mainly uninsured, underinsured, and publicly insured patients and provides primary care, dental, vision care, podiatry, and mental health services
ACCESS (Arab Community Center for Economic and Social Services)
A community-based organization with locations concentrated in Dearborn, MI, that provides community-based health care services, integrated behavioral health, and a range of educational programs that focus on disease prevention and health promotion
Some of the eligible workshop participants were leaders in government or community health. These individuals did not have the capacity to participate in the four workshops due to other commitments. Therefore, we engaged these individuals using a semi-structured interview format. The analysis and insights in this report are provided separately for the workshops and the interviews.
It is important to note that due to a variety of reasons, which we elaborate on in the insights section below, we undertook a targeted recruitment approach to engage Black Muslims using the same inclusion criteria above with the additional criteria of being racialized as Black. Our recruitment efforts involved reaching out to key influential leaders and community members in the local African American community, setting up a separate set of workshops that would be facilitated by an African American leader, and extending the recruitment period. It was important to make this effort because the lived experience of racialized individuals, whether Black, South Asian, or Arab American, are not the same, regardless of whether they share the same religious identity. Despite these efforts, we were only able to recruit two African American Muslim leaders for this study. One individual participated in the workshops, and another individual participated in an interview.
The study protocol received approval from the WCG Institutional Review Board (IRB) and was conducted in accordance with ethical guidelines for human subjects research.
The local steering committee had four members: three committee members were administrators from the HUDA Clinic (n=2) and ACCESS (n=1) and one was a local community leader with a health research background. The committee met four times over the course of the study. A charter and a communication plan was developed to take into account the capacity and interests of the steering committee members. The meetings focused on gathering feedback on the format and timeline of the workshops, identifying potential workshop participants, reviewing the initial findings of the workshops, and gathering insights on dissemination strategies. Local steering committee members were compensated at a rate of $50/meeting.
Potential participants (n=28) were invited to attend the workshops based on the participant recruitment strategy. Initially, 10 individuals agreed to attend but, ultimately, 7 individuals attended the four workshops, which were held in-person (workshop #1, #3, and #4) and online (workshop #2). Some of the reasons given by those who initially agreed to participate but then backed out were misunderstanding the time commitment, lack of childcare, change in job status, and limited availability on weekends.
The workshops consisted of individuals from diverse backgrounds based on ethnicity, race, and professional experience. Out of the seven participants, three were women and four were men, four were South Asian, two were Arab, and one was African American. One participant was from the education sector, three participants were from the healthcare sector, two participants were medical students, and one participant was in public health administration. Three of the participants held senior or executive-level positions within their place of work.
We organized four half-day long workshops from December 2023 to March 2024 (i.e., every second Saturday of the month) and participants were compensated $100 for each workshop.The purpose of these workshops was to generate new insights using systems thinking and system dynamics. Systems thinking is a way of thinking about the parts of a system and how they interact with each other to change the larger system. In the context of access to health care, the parts of the system are the factors associated with access to health care, and the larger system consists of access to health care services and the healthcare system. Based on this example, system dynamics is the way in which the system shifts in response to changes in some or all parts of the system (e.g., lower trust in a health care provider results in less chances of a patient coming back to that provider, higher levels of racial discrimination by a public health system leads to a decrease in the level of trust placed in the public health system by individuals or whole communities). The workshop activities and outputs (digital versions) are available in the Supplementary Materials. Workshop outputs in the main text of the report are intended to be examples and readers who want to view the diversity of workshop outputs should review the entire Supplementary Materials document. The facilitation guide for the first workshop (see Supplementary Materials) might be helpful for others interested in applying our approach to a complex and challenging topic facing their community.
In addition to the workshops, we conducted semi-structured interviews online with leaders in government and community health. The purpose of these interviews was two-fold. First, we validated some of the findings from workshop #1 regarding the problem statement, initial policy options, and key stakeholders. Validating these workshop outputs with the interviewees was important because the sectors they represented were not included in the workshops. For example, although we had a workshop participant who was a public health leader at a county health department, the perspective of a local health department leader was missing from the workshop. Similarly, we did not have anyone who represented the perspective of the City of Detroit and, therefore, interviewing an individual who worked in a public health-adjacent role within the City of Detroit was important to include in the study. The format of the interview was as follows. We presented to interviewees an overview of the project and digital versions of the outputs from workshop #1. We asked interviewees to review the materials presented for anything that was missing, should be added, or needed clarification based on the problem statement finalized by the workshop participants.
We created a digital version of outputs from each workshop activity and added relevant information, such as the number of votes, as applicable. For some activities, such as reviewing the feedback loops, we supplemented the digital version of each loop with relevant programs and initiatives based on the landscape analysis and participant input. Additionally, we derived insights from each of the workshop outputs and gathered data from multiple sources to corroborate the insights. The data sources we reviewed included the 2020 Decennial Census and American Community Survey from the U.S. Census Bureau, the PLACES data from the Centers for Disease Control, Area Health Resource File from the Health Resources and Services Administration, and the Environmental Justice Index from the Environmental Protection Agency. Using these sources, we developed a map highlighting multiple layers of information, including the locations of mosques in Southeast Michigan (a proxy measure for the residence of Muslim populations), areas of high social vulnerability, and limited access to healthcare services.
We recorded each online interview, and study team members summarized the responses of interviewees in a written document. In workshop #3, we presented these summary responses to the workshop participants along with information on the names, titles, and organizational affiliations of the interviewees. The workshop participants had the final say in what pieces of information and suggestions from the interviewees should be used to revise workshop outputs. This approach for integrating perspective between workshop participants and interviewees who did not attend the four workshops honored and prioritized the perspectives of workshop participants.
Tables S2 and S3 in the Supplementary Materials provide an overview of the activities conducted within each workshop including the purpose and output(s) of each activity. The following narrative summary identifies the main insights from workshop activities. We first identified the hopes and fears of workshop participants regarding this study. While the participants were hopeful that the overall study would have a practical and positive impact, they also feared that it lacked relevance to the broader community and that its scope and impact would be limited. In particular, participants raised concerns that an insufficient number of sectors were being represented among the workshop participants. For example, leaders or representatives from nonprofit organizations, patients and family advocates, immigrant and refugee communities, and policymakers were not represented in the workshops.
The problem statement for the workshops was “Which factors affect access to healthcare experienced by Muslim communities in Southeast Michigan?.” This statement was broad in scope and developed by workshop participants (Table S1 in Supplementary Materials), which might reflect the additional space participants wanted to give themselves since they feared that an insufficient number of sectors were represented at the workshop.
The problem statement developed by workshop participants: “Which factors affect access to healthcare experienced by Muslim communities in Southeast Michigan?”
As a result of the broad scope of the problem statement, it was not surprising that the participants came up with 36 key stakeholders with varying levels of power and interest to address their problem statement (Fig. 1). Prominent categories of key stakeholders included elected officials (e.g., City of Detroit Mayor Mike Duggan), healthcare systems and community health centers (e.g., Detroit Wayne Integrated Health System, Henry Ford Health), social and human service providers (e.g., Zaman International, Gleaners Food Bank), advocacy groups and community-based organizations (e.g., CAIR Michigan, Muhsen), and educational institutions (e.g., Miftaah Institute, local Muslim Students Association chapters). The interpretation of key stakeholders with low interest and high power (e.g., local media) is that these stakeholders have little interest or concern for the problem statement (i.e., factors associated with access to healthcare experienced by Muslim communities in Southeast Michigan). On the other hand, these stakeholders have high levels of power and influence over the factors associated with access to healthcare and could effectively and quickly address those factors.
Figure 1. Power vs. interest graph of key stakeholders based on the problem statement that was developed by the GMB workshop participants. Power in this context refers to the level of agency and influence, and interest refers to the level of interest of the key stakeholder to directly or indirectly address the problem.
This graph provided three key insights:
Based on the problem statement and key stakeholders, the workshop participants came up with 26 initial policy options that key stakeholders might consider to address the problem statement, including promoting mental health literacy in K-12 schools, enabling immigrants to obtain Medicaid regardless of their immigration status, enforcing charity care policies among all hospitals and expanding to new immigrants, offering free/reduced-price meals in schools, and free food delivery to food insecure patients. These policies were grouped into eight broader policy topics. For examples of policy topics, see Table 3; for a full list of policy topics and specific policies, see Tables S10 – S17 in Appendix III. After reviewing these broader policy topics, it became clear that the participants had identified policies that fit into either the social determinants of health or the public health/healthcare system. The public health system includes local and state health departments that strive to promote and protect the health of individuals and communities to give them a safe place to live, learn, work, play, and pray. The healthcare system includes hospitals, free clinics, and community health centers that serve the medical needs of patients in emergency, outpatient, and inpatient settings.
While some of the policies (see see Tables S10 – S17 in Appendix III) might seem unlikely or unrealistic, they served to highlight how we might address the problem rather than how we are currently addressing the problem of access to health care. This distinction is important because closing gaps in outcomes (e.g., disparities in emergency department utilization between foreign-born Arab Americans and U.S.-born white Americans) or shifting outcomes in a positive direction (e.g., increasing the number of American Muslims receiving mental health treatment) requires multiple parts of the larger system to work together by considering and implementing a range of policies rather than one single policy.
Participants identified variables of interest (see Table S7 and Fig. 2) that might be relevant to the key stakeholders and could be measured to see the impact of specific policies. Variables were identified through a series of workshop activities, such as the connection circle exercise. The relationships between these variables were organized visually in a causal loop diagram (Fig. 2). To better understand how to read this diagram, consider the example of the employment-based health insurance loop (top left in Fig. 2). This loop essentially suggests the following set of the statements:
The causal loop diagram was used to identify multiple feedback loops, and each feedback loop was named by workshop participants. Workshop participants also linked policies to feedback loops. This was an important linkage because it helps key stakeholders identify how they might slow or break down a feedback loop that leads to negative outcomes (e.g., in the employment-based health insurance loop example, rising unemployment rates would negatively affect the number of people insured through an employer). Table 3 provides examples of two feedback loops and related policies, key stakeholders, and existing programs/initiatives. Tables S10 – S17 in Appendix III provide similar information for all the feedback loops identified in the workshops.
The information in Tables S10 – S17 in Appendix III simplifies the complexity of the causal loop diagram (Fig. 2) into meaningful and easy-to-understand language for key stakeholders. One way to understand the information in Table 3, and similarly the more complete version in Tables S10 – S17 in Appendix III, is as follows.
Several insights emerged from reviewing the feedback loops and associated policies in Tables S10 – S17 in Appendix III and Figure 2.
First, there were three main categories of feedback loops: social determinants of health, racism and discrimination, and public health prevention and healthcare systems factors. These three types of feedback loops were different yet similar. They were distinct in the sense that different sets of key stakeholders might be interested in addressing them. For example, food banks, community-based organizations, and social service agencies would be more likely to address the social determinants of health and work with local mosques and Islamic centers than healthcare systems that lack the resources to address social determinants of health. The types of feedback loops were similar in the sense that there was overlap in policies (e.g., access to healthcare and health literacy) and relevant current programs and initiatives (e.g., Michigan Model for Health and ACCESS) needed to break the cycle of negative outcomes due to feedback loops. The key takeaway from this insight is that there are multiple pathways to address an outcome or variable of interest to American Muslim communities and key stakeholders in the health and healthcare system. The challenge is to identify those outcomes or variables of mutual interest and use the information in Tables S10 – S17 in Appendix III and Figure 2 to develop a shared understanding of which pathway to follow (i.e., which feedback loop to focus on). Once this shared understanding exists by clearly identifying the feedback loop(s) of interest, then it might be possible to identify existing programs and initiatives or develop new ones to collaboratively address the outcomes of mutual interest. This is one example of how a system approach might help American Muslim communities address big, complex challenges.
Second, the variable “trust in health care professionals” was the only common variable across the three types of feedback loops. This is not surprising and has been found in several other studies focusing on American Muslims (15, 23–26), the general public (27), and minoritized populations (28,29). Among American Muslims, the diversity of their backgrounds and experiences with discrimination due to race, ethnicity, religious practice and clothing, gender, sex, legal status, and socioeconomic status also plays a role when it comes to trust in health care professionals.
The central importance of trust in health care professionals provides an important insight from a systems perspective—it is insufficient for key stakeholders to address only one type of feedback loop. Instead, all feedback loops should be addressed to the extent possible. This is best illustrated by imagining a tricycle. The tricycle only moves forward as fast as it can when all three wheels are rotating in the same direction and at the same time. If two wheels are moving forward and the third wheel is moving backward or not moving at all, then there might be some progress in the right direction, but it is not moving as quickly as it would if the third wheel was also moving in the forward direction.
Applying this analogy to the three feedback loops (i.e., the wheels), it is easier to see that key stakeholders must address all three types of feedback loops: social determinants of health AND racism and discrimination AND public health prevention and healthcare systems factors. Addressing only the social determinants of health, for example, will increase trust in health care professionals but not as much as when stakeholders also address the other two types of feedback loops. While this is the ideal scenario, the lived experience of communities is often not ideal. Therefore, it is best for a community to address the three types of feedback loops at the same time to whatever extent possible based on their level of resources and capacity instead of addressing only one type of feedback loop or addressing the feedback loops in a sequence (e.g., first addressing social determinants of health, second racism and discrimination, and last public health prevention and healthcare factors).
Lastly, we identified specific key stakeholders who might be able to address the feedback loops in this study through specific current policies or programs. Tables S10 – S17 in Appendix III provide a comprehensive list of such policies and key stakeholders for each of the six feedback loops that were identified by workshop participants. The format of this information provides a customized way to share research findings back with the community and makes it easy for them to access the research and advocate to key stakeholders in a sustainable and practical manner. There are several ways different key stakeholders may use the information in Tables S10 – S17 in Appendix III to be empowered as a Muslim community in Southeast Michigan with sustainable and practical tools to advocate for solutions to healthcare access.
In addition to the GMB workshops, the insights from interviews with leaders in government and community health added important nuance and additional insights apart from what was learned from the workshop participants. Furthermore, the interviewees validated the workshop outputs, which was reassuring given the smaller than intended sample size of the GMB workshops. The following quotes capture their excitement for the project.
“Wonderful—[a] generational loop that needs to be broken such as stigma, so excited for this effort. ” —Quote from an interviewee
“Impressed with the scope—detailed, broad range of policy outcomes, rooted in community, built on the experiences of people. Intrigued.” —Quote from an interviewee
Interviewees identified some important key stakeholders such as ACCESS, Dearborn Department of Public Health, foundations and funders (e.g., Kresge Foundation, Ford Foundation), American Moslem Society (in Dearborn, MI), and Wayne Regional Educational Service Agency. Interviewees also identified several additional policy categories and specific policies including the following:
These insights added nuance to the feedback from the workshop. The suggestion of health diplomacy as a policy option, while similar, was distinct from the suggestion by workshop participants for health literacy as a policy option. While health diplomacy and health literacy fall under health communication, who practices them and in what setting is nuanced and important to highlight for American Muslims. Health diplomacy has to do with how, who, when, and what health information, programs, and policies are communicated to the public; health literacy focuses more so on the comprehension of the audience receiving the health information. Based on the feedback from the interviewees, health diplomacy seems to be more important for leaders in public health and healthcare, whereas health literacy was important to care coordinators, community managers, and community health workers. In Southeast Michigan where American Muslims are in positions of public health and healthcare leadership, a greater emphasis on health diplomacy might be more important than in other parts of the U.S. where American Muslims are not in such leadership positions. In this latter setting, health literacy would be the policy option with the greatest impact compared to health diplomacy.
Another nuance, which was not surprising given that the interviewees were public health leaders, was the identification of public health and healthcare organizations. Casting a wider net on the experience and level of organization where interviewees were situated within an organization enabled the identification of additional key stakeholders. These key stakeholders—such as ACCESS, Dearborn Department of Public Health, and foundations and funders—likely have high power and high interest but are not necessarily connected to those with similar levels of power and interest that were identified by workshop participants. The nuance here is that sometimes even leaders in public health, healthcare, mental health, and other spaces might not be aware of connections to other organizations with shared values and populations of interest. Not knowing which programs and initiatives are available or being organized by other organizations working within the same geographic region is a common issue in multiple sectors. The workshop outputs from this study might urgently help to address this issue by linking programs and initiatives to specific policies, stakeholders and feedback loops (Tables S10 – S17 in Appendix III). This would raise greater awareness among more key stakeholders regarding how best to leverage existing resources and programs to address inequities in access to health care among American Muslims in Southeast Michigan.
Taking these insights together from workshop participants and community leaders, we have the following recommendations for American Muslim communities in Southeast Michigan, particularly Arab American and South Asian populations, as they advocate for and seek to access, use, and receive high-quality healthcare.
Recommendation #1: Design and implement new ways to increase the ability of American Muslims to access, afford, and trust the healthcare system. Stakeholders should pursue this goal while supporting ongoing efforts that address approachability (e.g., translation services), accommodation (e.g., halal status of food and medication), and appropriateness (e.g., care provided by a provider the same gender as the patient) of health care services. For example, it is not simply the availability of translation services but the ability of patients to engage with the healthcare system through translators that should be the priority of healthcare systems and translation service providers. Similarly, the ease and quality of communication between healthcare office staff and patients is just as important as the religious accommodations for Muslim patients (e.g., gender concordant care).
Recommendation #2: Design and implement prevention strategies that prioritize the demographics, immigration experience, and socioeconomic makeup of neighborhoods. Neighborhoods are geographic areas perceived by residents who have a shared identity, rather than arbitrary administrative boundaries (e.g., census tracts). We provide suggestions of existing strategies that may be implemented to address specific feedback loops (see Tables S10 – S17 in Appendix III).
Recommendation #3: Address hard-to-reach and minoritized populations. State and city health and human service organizations (e.g., health departments, community action agencies), community health centers (e.g., federally qualified health centers, free clinics serving Muslims and other community groups), and community mental health agencies and treatment providers should build on existing partnerships and explore new opportunities that focus on innovative, diplomatic approaches to addressing health literacy, health misinformation, and health communication among hard-to-reach and minoritized populations. This might be accomplished through strengthening capacity to support health fairs, webinars, and educational initiatives at mosques, cultural centers, and other centers of community.
Recommendation #4: Increase the number of Muslim community health workers (CHWs). Stakeholders can raise awareness of educational pathways to public health and healthcare professions and build sustainable collaborations with agencies who employ Muslim CHWs who are already serving Southeast Michigan American Muslim communities. CHWs are often trusted individuals within the communities they serve.
Recommendation #5: Holistically address social determinants of health. Community-based organizations that assist Muslim patients and clients with health-related social needs, such as food insecurity, transportation, and rent assistance, should partner with the regional initiatives (e.g., Community Information Exchange, Wayne County Community Action Agency) to holistically address social determinants of health.
Recommendation #6: Build bridges with community organizations, healthcare systems, and local governments. Local Muslim religious centers and community-based organizations should continue to build intentional bridges with public and community health organizations, hospitals, community-based organizations, and city/county governments that focus on social determinants of health, access to care, and specific health outcomes, such as mental health, maternal and child health, chronic diseases, and elderly care.
