
Erum Ikramullah and Sarah Baker
Recent polling from Gallup reveals that adults in the United States continue to show declines in self-reported mental health since a recent peak in 2019 prior to the pandemic. In 2025, for the first time ever, the proportion of U.S. adults who rate their mental health as “excellent” fell below 30%. The American Psychiatric Association found that adults in the U.S. are feeling increasingly anxious in their annual mental health poll, fielded in 2024. In that poll, 43% of adults reported feeling more anxious than they did the previous year, up from 37% in 2023 and 32% in 2022.
While these studies provide an overall view of mental health among adults in the U.S. and even include demographic breakdowns, they do not provide specific data on mental health across faith communities. The Institute for Social Policy and Understanding (ISPU) seeks to fill this gap by providing data on the mental health of Muslim in the United States, relative to other faith communities and those not affiliated with a religious group. Understanding the mental health of Muslims in the United States is crucial for both Muslim community leaders and health professionals looking to tailor services to meet community needs. It’s also paramount for health professionals more broadly, who serve diverse communities and patients. Muslim communities in the United States have a set of demographics and experiences linked to greater risk or vulnerability for poorer mental health outcomes.
ISPU’s American Muslim Poll 2025 shows that Muslims tend to be younger than the general public and all other faith and non-faith groups, with about one quarter of Muslims being between the ages of 18-29 compared to 5%-15% of all other groups. Recent studies on the U.S. population find that clinical diagnosis of depression and anxiety are higher among adolescents and young adults than older age groups and that symptoms often persist into adulthood. Additionally, American Muslim Poll 2025 finds that Muslims in the United States remain the most racial and ethnically diverse religious group and the only group with no single majority racial/ethnic group. Specifically, 28% of Muslims in the U.S. identify as Black or African American, 20% identify as white, 24% identify as Asian, 12% as Arab, 9% as Hispanic and small proportions of other racial/ethnic groups. Decades of prior research show that racial and ethnic minorities in the U.S. are vulnerable to worse mental health outcomes, often due to lower access to care and also higher exposure to the stress of discrimination and racism.
In 2025, ISPU found that Muslims in the US report higher levels of religious discrimination compared with other faith communities and that Islamophobia is also on the rise. Islamophobia has been shown to be a structural determinant of mental health for Muslims in the United States. Similarly, research shows that low-income Americans are at greater risk for poor mental health outcomes due to the chronic stress exposure that comes with lower socioeconomic status as well as having high barriers to receiving sustained treatment. American Muslim Poll 2025 finds that 35% of Muslims in the United States have a household income of $30,000 or lower, making them the religious group most likely to do so (other groups range between 11%-20%).
Finally, 40% of Muslims in the United States were born outside of the U.S. Thus a significant share of Muslims are immigrants or refugees and face the stress and fear of living in the United States at a time when immigrants and refugees are under threat from the U.S. government. The individual and combined demographics and experiences of Muslims in the United States show their elevated risk of chronic stress which leads to a higher prevalence of mental health disorders, as well as systemic barriers to accessing the treatment needed to recover.
Among Muslim communities there are also barriers to treatment from mental health professionals such as stigma, mistrust in the healthcare system, and reliance on other coping mechanisms. ISPU’s Community in the Time of Corona study found that Muslims reported similar levels of mental distress as the general public, but were more likely to rely on faith and family to cope, rather than professional treatment.
This analysis uses data from ISPU’s American Muslim Poll 2025 to provide nationally representative data on Muslims in the United States regarding mental health to inform and support the work being done to improve outcomes for Muslims across the country. The full methodology is available here. We explore differences by gender, age, and race/ethnicity, based on prior research showing demographic differences in prevalence and experience of mental health conditions and treatment seeking.
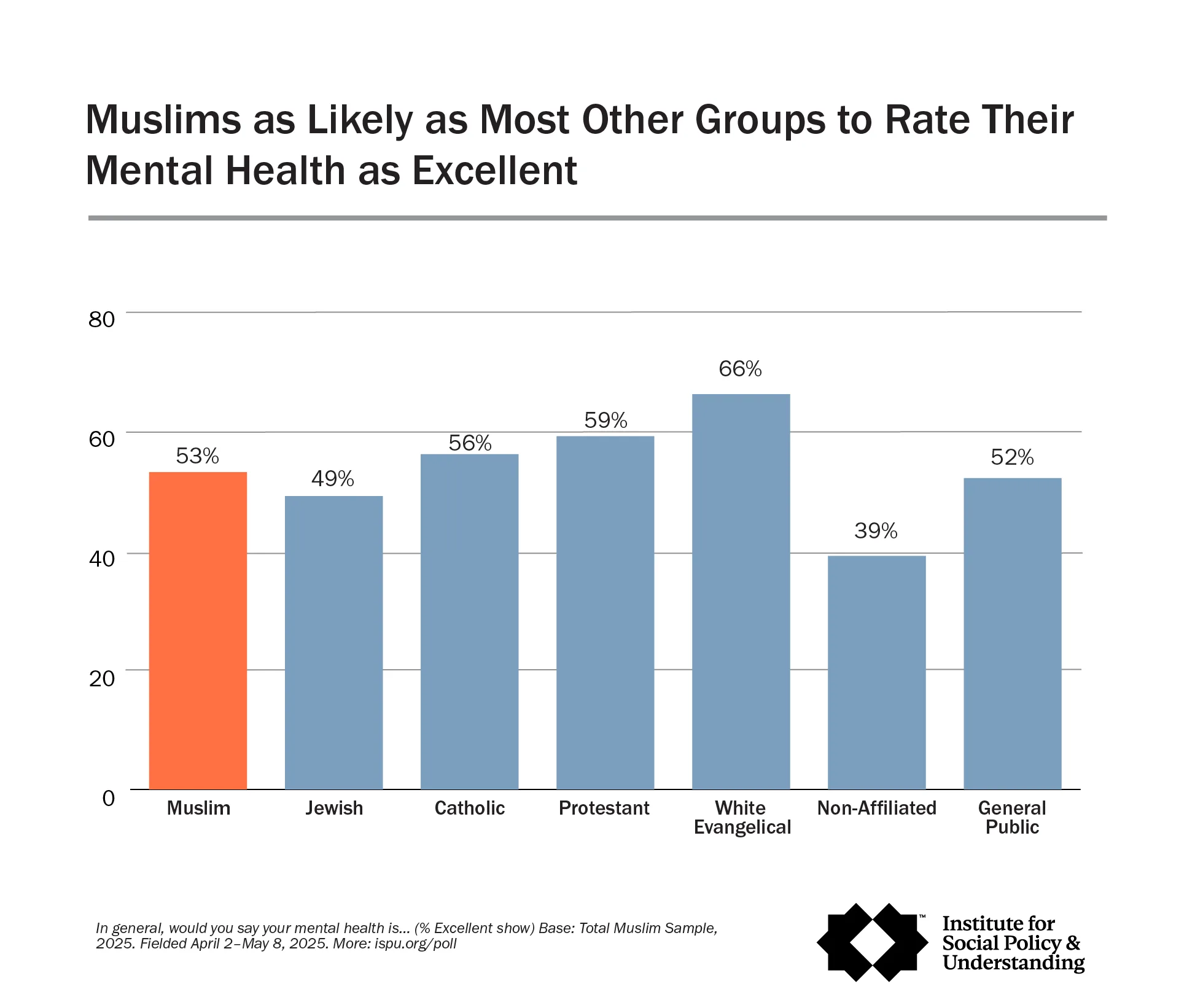
A slight majority of Muslims rate their mental health as “excellent” or “very good,” on par with most other groups.
When asked about their mental health, slightly more than half of Muslims (53%) report having “excellent” or “very good” mental health, on par with 49% of Jews, 56% of Catholics, 59% of Protestants, and 52% of the general public. White Evangelicals (66%) are more likely than Muslims to report “excellent” or “very good” mental health while those not affiliated with a religious group are less likely (39%). One quarter of Muslims rate their mental health as “good,” on par with most other faith communities. Muslims (25%) are on par with Catholics (27%), Protestants (28%), and white Evangelicals (25%) in rating their mental health as “good.” Muslims are less likely than the general public (30%), Jews (34%), and the non-affiliated (35%) to report their mental health as “good.”
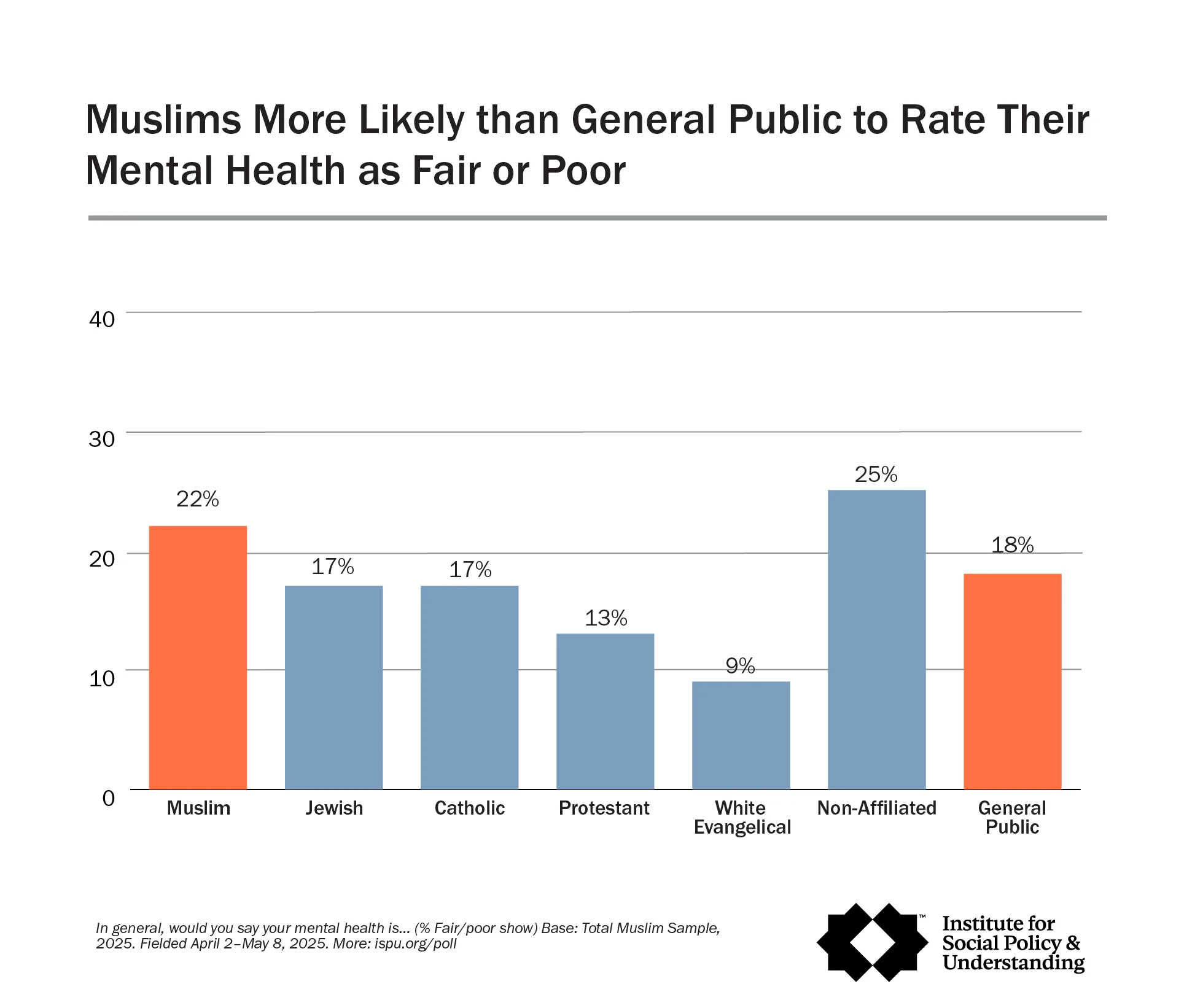
Muslims are more likely than the general public, Protestants, and white Evangelicals to rate their mental health as “fair” or “poor.”
More than one-fifth (22%) of Muslims rate their mental health as “fair” or “poor,” more likely than the general public (18%), Protestants (13%), and white Evangelicals (9%) to rate their mental health as “fair” or “poor.” Muslims are as likely as Jews (17%), Catholics (17%), and the nonaffiliated (25%) to say their mental health is “fair” or “poor.”
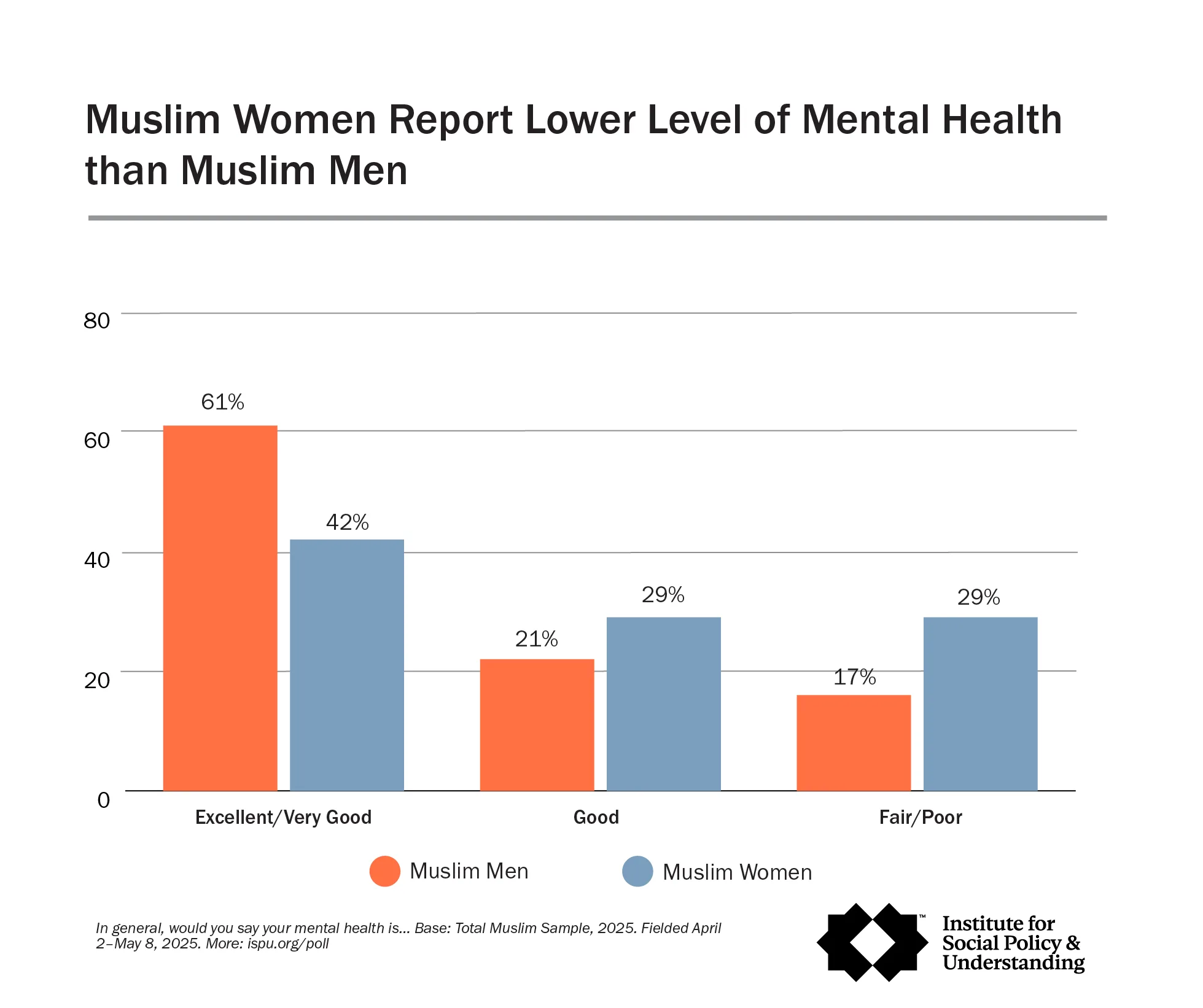
Muslim men report their mental health more positively than Muslim women.
Sixty-one percent of Muslim men say their mental health is “excellent” or “good”, compared with 42% of Muslim women. We find a similar pattern of men more likely to report excellent/good mental health compared to women among Protestants (71% vs. 48%), white Evangelicals (80% vs. 54%), and the general public (59% vs. 44%).
On the other hand, Muslim women are more likely than Muslim men to rate their mental health as “fair” or “poor” (29% vs. 17%). The same pattern holds among the general public with 21% of women vs. 14% of men reporting fair/poor mental health as well as among the non-affiliated (31% of women vs. 18% of men). Muslim men and women are equally likely to rate their mental health as “good” (21% of Muslim men and 29% of Muslim women).
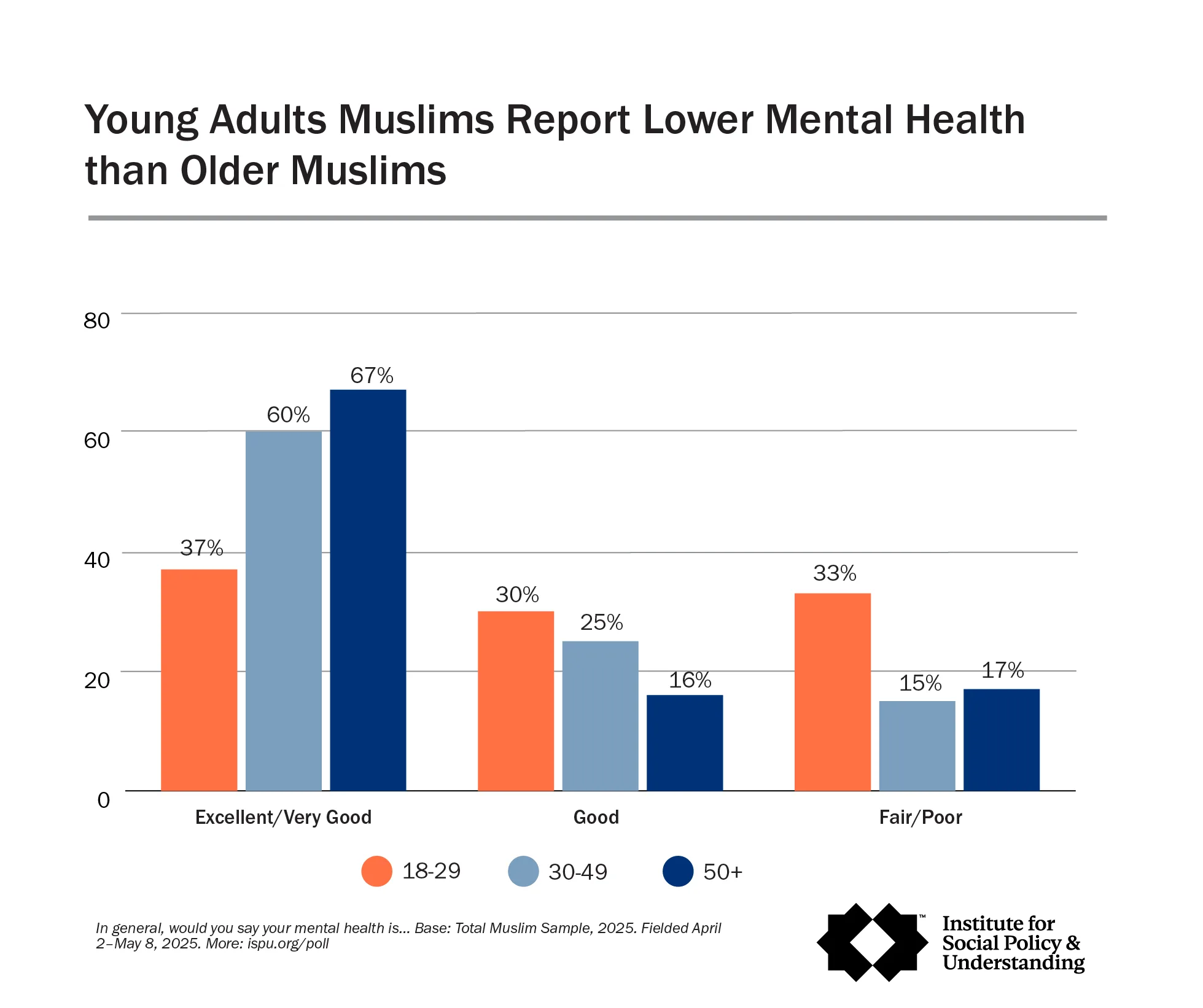
Young Muslims report lower levels of mental health.
Thirty-seven percent of Muslims 18-29 report “excellent” or “very good” mental health, compared with 60% of Muslims 30-49 and 67% Muslims aged 50+. Among the general public, 39% of 18-29 year olds and 39% of 30-49 year olds vs. 66% of 50+ say their mental health is “excellent” or “very good”. Young adult Muslims are about twice as likely as older Muslims to rate their mental health as “fair” or “poor”. Thirty-three percent of Muslims 18-29 report “fair” or “poor” mental health, compared with 15% of Muslims 30-49 and 17% of Muslims 50+.
White Muslims report more positive mental health than Muslims of other racial/ethnic groups.
White Muslims (69%) are more likely than Black (51%), Asian (46%), and Arab (40%) Muslims to rate their mental health as “excellent” or ‘good.’ Among the general public, white Americans (57%) are more likely than Hispanics (40%) to report excellent/good mental health. About half, 51%, of Black Americans report their mental health as “excellent” or “good”.
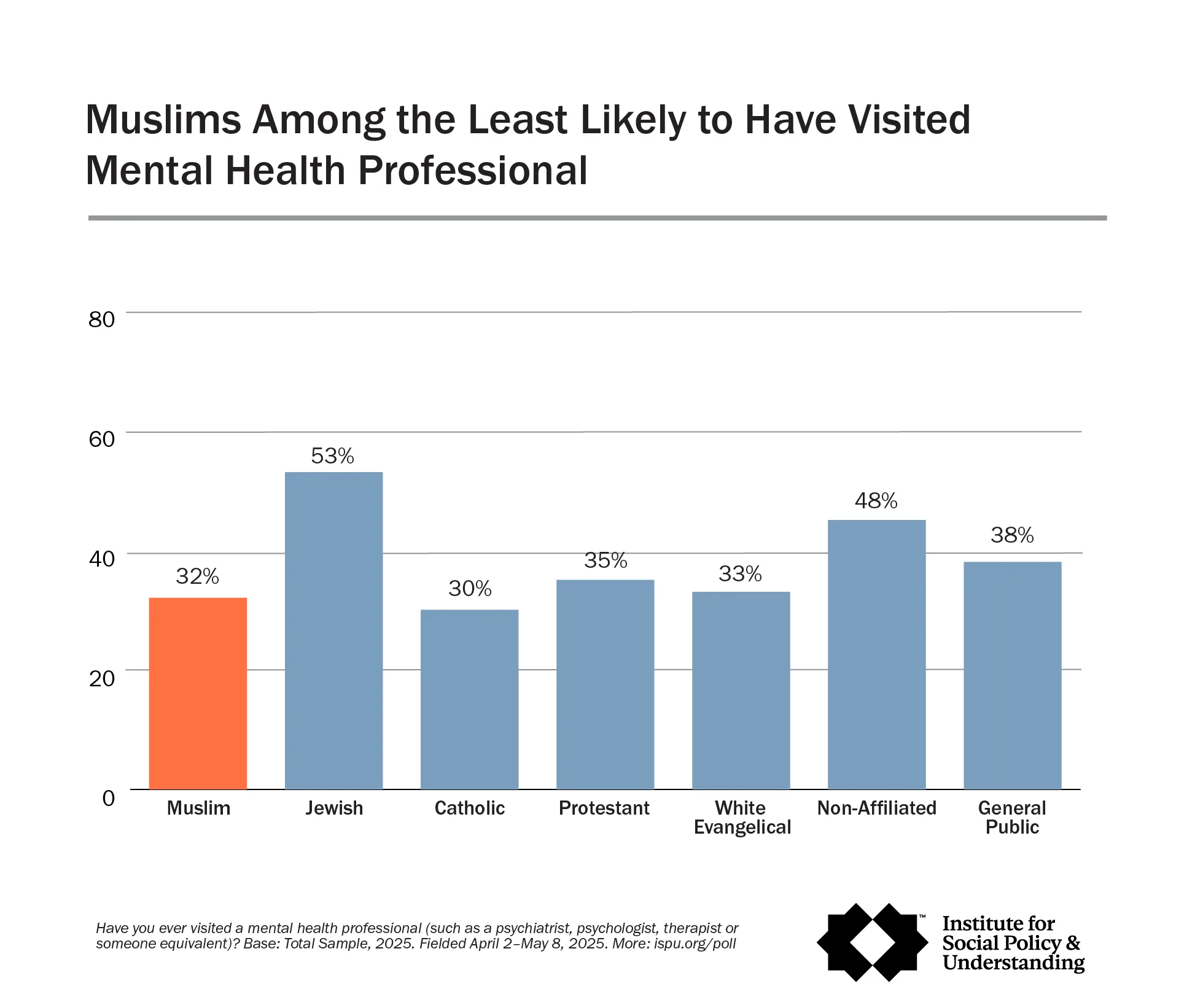
Muslims less likely than general public to have ever visited a mental health professional.
When asked whether they had ever visited a mental health professional, Muslims (32%) were less likely than Jews (53%), the non-affiliated (48%), and the general public (38%) to report having done so. However, they were equally as likely as Christian groups, including Catholics (30%), Protestants (35%), and white Evangelicals (33%). Notably, the proportion of Muslims who have ever visited a mental health professional has grown over the past few years, rising from 25% in 2019 to 32% in 2025.
Muslim men and women are on par in having seen a mental health professional.
Muslim men and women were equally likely to have visited a mental health professional (28% and 36%, respectively). Among other groups, women were consistently more likely than men to report having done so, including Jews (63% vs. 44%), Protestants (46% vs. 23%), white Evangelicals (44% vs. 20%), and the general public (44% vs. 31%).
For Muslims, no significant difference by age in having ever visited a mental health professional.
For Muslims, there was no significant difference by age in having ever visited a mental health professional. This was not the case for the general public, where those aged 30-49 were more likely to have ever visited a mental health professional than those 50 and older (44% vs. 33%).
Black Muslims more likely than Asian Muslims who have ever accessed a mental health profession (42% vs. 23%).
Black Muslims were more likely than Asian Muslims to have ever visited a mental health professional (42% vs. 23%). Among the general public, white Americans were more likely than Hispanic Americans to have done so (41% vs. 31%).
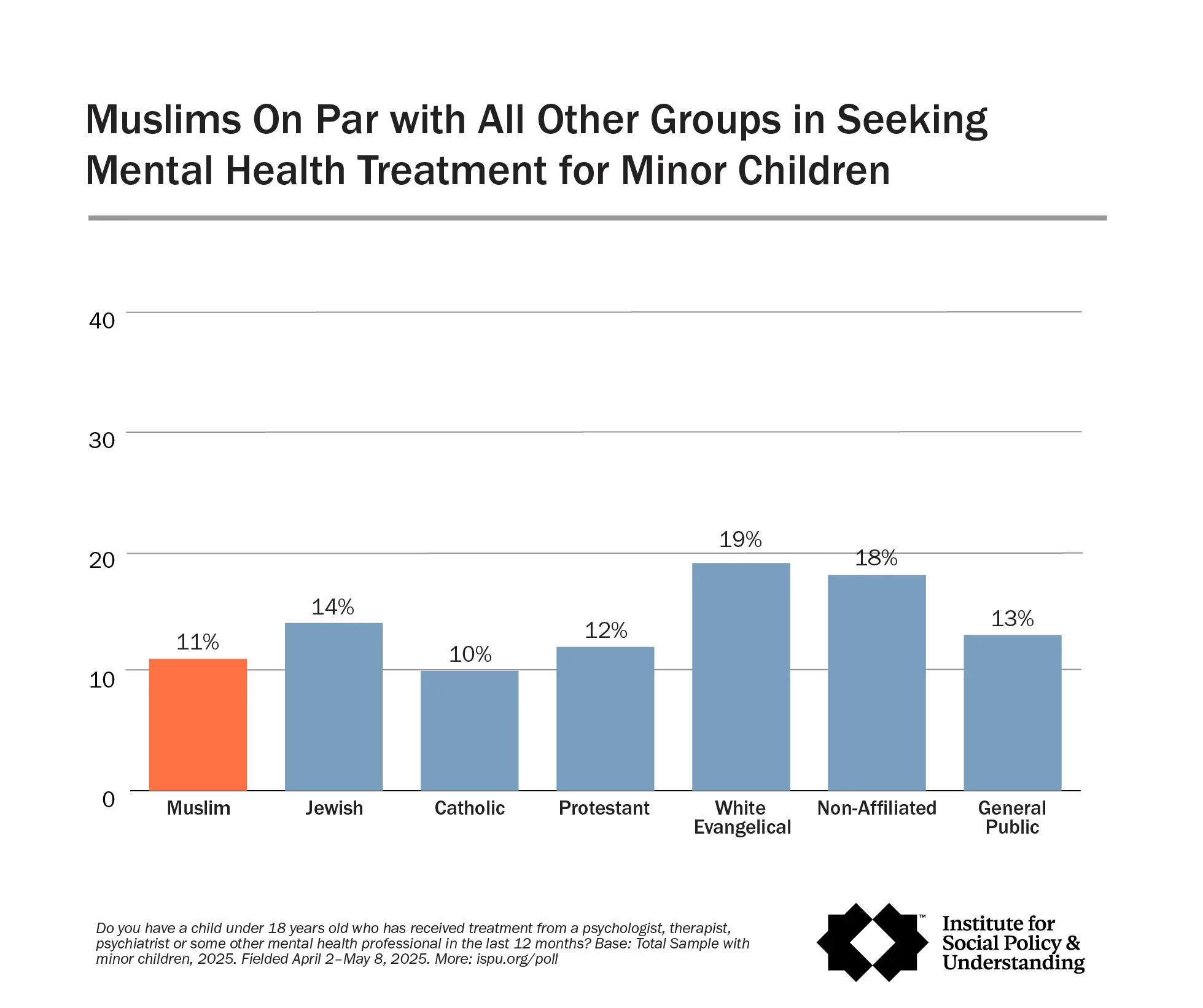
Muslims as likely as others to report having a child under 18 who has received treatment from a mental health professional.
While Muslim adults were among the least likely to seek professional mental health treatment, they were just as likely as other groups to report having a child under 18 who has received treatment from a mental health professional (11%), including Jews (14%), Catholics (10%), Protestants (12%), white Evangelicals (19%), the non-affiliated (18%), and the general public (13%). Further research is needed to better understand generational patterns of mental health treatment seeking among Muslims in the United States.
Data from ISPU’s American Muslim Poll 2025 reveal mixed findings on Muslim mental health. While Muslims report similar levels of positive mental health compared to Jews, Catholics, Protestants, and the general public, they are more likely than several of these groups to rate their mental health as “fair” or “poor.” Disparities also exist within the Muslim community, with Muslim women and younger Muslims reporting lower levels of mental health than their male and older counterparts. Research from the National Institute of Mental Health also found that women and younger people are more susceptible to negative mental health outcomes. These findings become more urgent when considered alongside the demographic profile of American Muslims: a younger population with high levels of racial diversity, lower household incomes, and a substantial number of refugees and immigrants, each of which is associated with greater vulnerability to poorer mental health outcomes. The data also show that Muslims remain less likely than the general public to utilize mental health services, although this number has steadily improved from 2019, possibly due to emerging programs and efforts within the Muslim community. Institutions like Michigan State’s Muslim Mental Health Consortium, the Muslim Wellness Foundation’s Black Muslim Psychology Conference, Maristan, and Stanford’s Muslim Mental Health & Islamic Psychology Lab have provided research and education to address stigma and gaps in knowledge about mental health to Muslim communities. Continued research and targeted interventions are essential to address these persistent disparities and improve mental health outcomes across the Muslim community.
– Promote mental health education and awareness: Partner with mental health professionals to provide education to community members about mental health conditions, the harmful effects of stigma, and the particular vulnerabilities faced by specific groups among Muslims in the United States, including women, youth, racial/ethnic minorities, and immigrants.
– Enhance visibility of available mental health resources: Inform and connect community members to the range of mental health treatment options available in their area, with particular emphasis on culturally competent providers who understand the unique needs and values of Muslim communities.
– Build mental health service capacity within community spaces: Consider establishing mental health services directly within mosques and community centers to normalize the importance of mental wellbeing and remove barriers to treatment. For example, the Islamic Center of Detroit launched the first mental health clinic in its vicinity, My Mental Wellness Clinic, to ensure mental health care is visible, accessible, and affordable to its constituents. A study on the role of mosque communities in supporting Muslims with mental illness affirms that ‘integrating Muslim mental health professionals into the mosque community, and providing treatment services on-site can help normalize the use of these services and increase their accessibility.
– Understand and address barriers to mental health care access among Muslim communities: Conduct assessments to identify the unique barriers Muslim communities face in accessing mental health services, including cultural stigma, lack of religiously and culturally competent care, language barriers, and affordability concerns. Use these insights to develop targeted strategies that make mental health services more accessible, welcoming, and responsive to community needs.
– Collaborate across sectors to reduce systemic barriers: Partner with community organizations, mosques, research institutions, and social service agencies to create integrated pathways that address the barriers to mental health treatment. See ISPU’s recent report on the systemic factors that produce barriers in accessing healthcare services in Southeast Michigan for Arab and South Asian Muslims.
– Invest in religious literacy and cultural competence training: Pursue learning opportunities that build understanding of Islamic beliefs and practices, as well as the diverse cultural backgrounds within Muslim communities. This includes knowledge that addresses common mental health concerns among Muslims, including the impact of Islamophobia on mental wellbeing.
– Offer flexible and accessible service options: Provide accommodations such as gender-matched providers, virtual appointments, evening and weekend hours, and private spaces for prayer to reduce barriers and demonstrate cultural responsiveness.
– American Muslim Health Professionals (AMHP)
– The Family and Youth Institute (FYI)
– Institute for Muslim Mental Health
– Maristan
– Muslim Mental Health and Islamic Psychology Lab (MMHIPL) at Stanford University